
Antimalarial agents - Medicinal Chemistry III B. Pharma 6th Semester
Antimalarial agents
Contents
• Malaria – Etiology
• Life cycle of Malaria parasite
• Modern malaria chemotherapy
• Classification of Antimalarials
• Structural Activity Relationship, pharmacokinetics, pharmacological effects and side effects of the following:
Cinchona alkaloids
8- aminoquinolines
4- aminoquinolines
9- acridines
• Synthesis of chloroquine
• Synthesis of primaquine
• Synthesis of quinacrine
• Biguanides – biological transformation, SAR, metabolism, effects and side effects
• Pyrimidines – site of action, SAR
• Sulphones and sulphonamides – Action and toxicity
• Mechanism of action of Antimalarials
Learning Objectives
At the end of this lecture, student will be able to
• Discuss the etiology of Malaria
• Explain modern malarial therapy
• Classify Antimalarials
• Compare the structure and activity relations of Antimalarials
• Discuss the metabolism, effects and side effects of Antimalarials
• Explain the synthetic route for the synthesis of chloriquine
• Explain the synthetic route for the synthesis of primaquine
• Explain the synthetic route for the synthesis of quinacrine
• Compare the structure with that of activity of antimalarials
• Discuss the biotransformation of specified antimalarials
• Describe the action and toxic effects of antimalarials
• Explain the synthesis of certain antimalarials
Etiology
Etiology (study of the cause/ causation of disease or condition):
Malaria in humans is caused by four species of Plasmodium (protozoan parasite)
• Plasmodium Vivax (benign tertian malaria)
• Plasmodium falciparum (malignant tertian, sub-tertian malaria)
• Plasmodium malariae (quartan malaria)
• Plasmodium ovale (mild tertian malaria ovale tertian)
In other mammals, birds and reptiles it is caused by many other species.
Symptoms
• The disease is characterized by successive chills, fever and sweats.
• If the symptoms occur every 3rd day- Tertian, if it occurs every fourth day- Quartan
• All species of plasmodium have two hosts, a vertebrate and a mosquito that acts as both vector (carrier) and a definitive host.
• Vector for human malaria- Female ‘Anopheles’ Mosquitoe
• The sexual phase of life cycle begins when a female mosquito bites an infected vertebrate and ingests blood containing the malarial parasite in the gametocyte stage.
Life cycle of Malarial parasite
• Mosquito bites an infected vertebrate and ingests the malarial parasite
• In the stomach of the mosquito, the sexual phase of development called sporogony occurs.
• The male-female gametocytes form gametes. An ookenite (zygotes) is formed by fertilization and penetrates the stomach wall outside the stomach wall. Outside the stomach, oocysts are formed which produces sporozoites, that are released by the rupturing of the oocyst.
• The sporozoites travel to the salivary glands of the mosquito, from which they may be transferred to an uninfected vertebrate host by the bite of mosquito.
• Injected sporozoites disappear rapidly from the blood of the vertebrate, entering the parenchyma cells of the liver and some other tissues. The parasite now begins the asexual phase of development called schizogony.
• In this pre-erythrocytic stage, the parasite grows and divides to form schizont. The schizont segment to form many merozoites, which causes the rupturing of the cell, beginning the erythrocytic stage.
• Within the red blood cells, the merozoites become trophozoites and multiplication occurs by schizogony .
• The schizonts formed from the trophozoites divide into merozoites and continuously increase the no.of merozoites available to invade more red blood cells, so that, finally the no. of rupturing cells is sufficiently great to initiate the symptoms of disease.
• The asexual cycle continues until chemotherapy is initiated, immunity is developed or death occurs.
• ‘The continuous invasion and subsequent rupture of erythrocytes lead to the development of another significant symptoms of malaria, anemia.
• When normal reproduction of the erythrocytes becomes unfavorable, some trophozoites from the erythrocyte stage develop into male or female gametocytes, which circulate in the blood to be available for ingestion by another mosquito.
Potential ways to control malaria
• Elimination of the vector-simplest, cost effective
Prevent contact with insect- a nocturnal feeder-use window screens, mosquito nets
Eliminate mosquito by application of insectidies & destroy breeding grounds
• Drug therapy-tremendous need for new, more effective drugs
Cause protozoa develop resistance by different mechanisms & there are a variety of adverse reactions. No single drug is effective against all species
• Vaccination- no effective vaccination has been developed
The parasite does not elicit an effective immune response. The only approved vaccine as of 2015 is RTS,S,-trade name Mosquirix. It has relatively low efficacy.
Possible sites for drug therapy
• Kill the sporozoites injected by the mosquito and/or prevent the sporozoites from entering the body
• Kill the primary schizonts in the hepatocytes and/or prevent them form becoming merozoites
• Kill the merozoits in the blood and/or prevet them from developing into gametocytes
• Kill the gametocytes before they enter the mosquito and fertilize into zygotes
Modern malaria chemotherapy
• Most drugs used in modern malarial chemotherapy as chloroquine, amodiaquine, pyrimethamine, quinine, sulfonamides act primarily at the erythrocytic stage, in the malaria life cycle (i.e. at site 4). Since the severe and life threatening clinical symptoms of malaria occur at the stage, these drugs are very useful in
1. Treating all four human malarias and
2. In preventing clinical symptoms of four human malarias.
• However, cures from these ‘site-4’ drugs can result only with P. falciparum - the other three species P. vivax, P. malariae and P. ovale have a ‘secondary exo-erythrocyte’ (secondary schizont) stage which can periodically release new merozoites for years or decades.
• An additional drug which is effective at the ‘site-3’ stage is usually primaquine.
• It is desirable to protect humans from initial infection by the mosquito at ‘site one’. But no drugs are available which are effective at this site.
• Primaquine is active at ‘site 2’, so it could be used as a prophylactic against all forms of human malaria, but due to its toxicity it cannot be used for a prolonged period.
• Primaquine is also effective as a gametocide (at site 5)
• The best means of controlling the spread of the disease is through community sanitation and use of insecticide.
• A complicating factor in modern malaria chemotherapy is that drug- resistant strains of plasmodia have been reported. Eg. Chloroquine resistant P. falciparum or P. vivax in one geographical area and quinine resistant P. falciparum in another.
Classification of Antimalarials
The important classes of antimalarial drugs are:
Cinchona alkaloids
4-aminoquinolines
8-aminoquinolines
9-aminoacridines
Biguanides
Pyrimidines (diaminopyrimidines)
Sulfones
Newer antimalarials
• Cinchona alkaloids
Quinine
Quinidine
Cinchonine
Cinchonidine
• 4-aminoquinolines
Chloroquine
Hydroxychloroquine
Mefloquine
Amodiaquine
• 8-aminoquinolines
Primaquine
Pamaquine
Pentaquine
• 9-aminoacridines
Quinacrine
Acriquine
• Biguanides
Proguanil
Chloroproquanil
Cycloguanil
• Pyrimidines
Pyrimethamaine
Trimethoprim
• Sulphones
Dapsone
• Polycyclic antimalarial drugs
Doxycycline
Halofantrine
• Newer antimalarials
Artesunate
Artemether
Atovoquon
Cinchona alkaloids
Eg. Quinine, Quinidine, Cinchonine, Cinchonidine.
The alkaloids are derivatives of 4-quinolinemethanol bearing a substituted quinuclidine ring system

SAR of Cinchona alkaloids
1. All four of the cinchona alkaloids are active antimalarials. Thus the 6-OCH3 group is not essential for activity.
2. The quinoline methanol portion becomes important in synthetic drugs.
3. All the alkaloids having same configuration at R1 & R2 are diastereoisomers, differing in configuration at 3rd & 4th chiral centers (C-8 and C-9)
4. Although all four alkaloids show antimalarial activity, their C-9 epimers (i.e. having either 8R:9R or 8S:9S configurations) are inactive.
5. Any modification of the 2˚ alcohol at C-9, through oxidation, esterification and similar processes diminishes activity.
6. The quinuclidine portion is not essential for activity; however, the tertiary (3˚) alkyl amine attached to C-9 is important. This forms the basis for the design of synthetic antimalarials.
Metabolism: -
• Quinine is metabolized in the liver to the 2’ – hydroxyl (carbostyril) derivative, followed by additional hydroxylation on the quinuclidine ring to provide the 2,2’-dihydroxy Derivative as the major metabolite.
• This metabolite has low antimalarial activity and is rapidly excreted.
• Excretion is mainly in the urine.
Effects: -
• The cinchona alkaloids act on the erythrocytic merozoites. They do not effect a radical cure but decrease symptoms.
• Quinine is used in treating some forms of malaria, in which resistance to other agents has developed.
• Also, cinchona alkaloids are antipyretic by the action on central temperature regulating mechanism causing peripheral vasodilation
Side effects: -
• Side effects include – skin allergies, deafness, vertigo (giddiness - dizziness) and slight mental depression.
• Quinine passes the fetal barrier and affects the vision of the new born.
Advantages: -
• Quinine is the drug of choice only for chloroquine resistant P. falciparum. The resistance to quinine has not developed as readily as it has to the synthetic drugs.
Quinoline analogues - 4-aminoquinolines

Chloroquine

Hydroxychloroquine

Amodiaquine

Mefloquine
SAR of 4-aminoquinolones
• The 3˚ amine is important for activity
• Side chain length (4-carbon) & 7-chloro-group are optimal for activity.
• Substitution of –OH gp on one of the ethyl group on the 3˚ amine reduces toxicity and increase the plasma concentrations (more effective) - a metabolite of chloroquine (hydroxyl chloroquine).
• Incorporation of an aromatic ring at the 3˚ amino gp, produces a compound of reduced activity and toxicity e.g amodiaquine
• Incorporation of a methyl group on C-3 on the quinoline ring decreases activity e.g santoquine
• Substitution of a methyl group on C-8 causes a complete loss of activity.
Absorption, Distribution and excretion:
• Chloroquine is absorbed readily from the G.I,T, but amodiaquine gives lower plasma levels than others in the group.
• Peak plasma concentrations are reached in 1 to 3 hrs, with blood levels falling off rapidly after administration is stopped.
• About half the drug in the plasma is protein bound.
• These drugs concentrate in the liver, spleen, heart, kidney & brain.
• These compounds are excreted rapidly with most of the unmetabolized drug being accounted for in the urine.
Uses
• These drugs are active against the erythrocytic forms of all malarial parasites leading to clinical cure.
• They do not prevent the disease and they are not active against the liver infecting forms.
• They are also used in the treatment of extra-intestinal amebiasis.
Toxicity
• The toxicity of 4-amino quinolone is quite low. The side effects include nausea, vomiting, anorexia, abdominal cramps, diarrhea, headache, dizziness, pruritus and urticaria
• Long-term administration in high doses may have serious effects on the eyes.
• Patients with liver diseases particularly should be watched when 4- aminoquinolines are used.
8-aminoquinolines
• 8-aminoquinolines, unlike 4-aminoquinolines, are active against the pre- or exo-erythrocytic forms of the malarial parasite.
• 8-aminoquinolines are reserved for prophylactic purposes and for the production of radical cure in infections due to P. vivax and P. malariae
SAR: -
• The 6-methoxy group is essential for activity
• Side chain carbon length can vary from 4 to 6 carbons
• The extent of substitution of the amino is not as critical and the drug of choice, Primaquine, is a primary amine.

Primaquine

Pamaquine

Pentaquine
ADME
• The 8-aminoquinolines are absorbed rapidly from the G. I .tract. Peak plasma concentrations are reached within 2 hours after ingestion after which the drug rapidly disappears from the blood.
• The drugs are localized mainly in the liver, lung, brain, heart and muscle tissue.
• Metabolic changes are produced in the drug very rapidly and on excretion, metabolic products account for nearly all of the drug.
• The antiplasmodial and the toxic properties of these drugs are produced by metabolic transformation products.
Toxicity: -
• The toxic effects are principally in the CNS and the hematopoietic system (system pertaining to the formation of blood cells).
• Other side effects are anorexia, abdominal pain, vomiting and cyanosis (a dark bluish colaration of skin and mucous membrane due to deficient oxygenation of the blood in the tissues), hemolytic anemia leukopenia (abnormal decrease in WBC<5000/cu.mm) and methemoglobinemia (condition in which more than 1% of hemoglobin is blood is oxidized to ferric form Fe+++)
Uses: -
Primaquine is used mainly to prevent relapses due to exo- erythrocytic forms of the parasites.
9-Aminoacridines
Act as schizonticides but are inferior to the 4-aminoquinolines
• Quinacrine hydrochloride (Mepacrine HCl)
• 6-chloro-9[{4-(diethylamino)-1-methylbutyl}amino]-2-methoxy acridine dihydrochloride.

Toxicity: -
• Extremely toxic - largely replaced by the 4-aminoquinolines
• The toxicity involves the CNS, blood and fatal drug reactions.
• The toxic effects include-convulsions, psychotomimetic (mental disturbances) reactions, aplastic anemia [decreased formation of erythrocytes and hemoglobin from aplastic(defective) bone marrow] and exfoliate (scabial) dermatitis
• A side effect of therapy is yellow pigmentation of the skin and yellow color in the urine.
Synthesis of chloroquine
• It is prepared by adopting the following four steps viz.,
• (a) Preparation of 4, 7-Dichloroquinoline (i.e., the nucleus)
• (b) Preparation of 2-amino-5-diethyl amino pentane, or 1- diethylamino-4-amino pentane (i.e.,the side chain).
• (c) Condensation of ‘a’ and ‘b’.
• (d) Addition of concentrated phosphoric acid to a hot ethanolic solution of the condensed product.
A) Prep. of nucleus

B) Prep. of side chain

C) Condensation of A and B

D) Prep. of phosphate salt

Synthesis of Chloroquine



Synthesis of Pamaquine
• Synthesis of the nucleus

• Condensation of the side chain and nucleus


• 8amino 6 methoxy quinolone reacts with 2 chloro diethyl amino pentane to form pamaquine.
Synthesis of Quinacrine
• Synthesis of the nucleus

• Condensation with the side chain

Biguanides
• Biguanides are prodrugs for their active metabolites-the dihydrotriazines (cyclized product)
• Biological transformation is illustrated with Proguanil (chlorguanide).
• The antimalarial agent formed in this instance is the drug cycloguanil, which itself is available as the pamoate salt, having a duration of action of several weeks to months.

Biotransformation of proguanil

SAR: -
• Substitution of a halogen on the para-position of the phenyl ring significantly increases activity e.g. Chlorine substitution in chloroguanil –
• The 4-bromine analog also is very active.
• A second chlorine at the 3-position of the phenyl ring of proguanil further enhanced the activity.
• However, the dichloro compound, chlorproguanil, is more toxic than chlorguanil.
Absorbtion, distribution and elimination: -
• They are absorbed very quickly from the GIT.
• They are concentrated in the liver, lungs, spleen & kidney but does not cross the blood brain barrier.
• 75% of the drug present in plasma is bound to protein
• They are metabolized and eliminated rapidly, mainly in the urine
• As a result, frequent administration of these drugs is necessary.
Toxicity: -
• Low toxicity, but with increased doses, haematuria (blood in urine) and albuminuria (albumin in urine) are observed
Effects: -
• These derivatives including cycloguanil are potent schizonticides against both exoerythroctic & erythrocytic forms of P. falciparum and P. vivax.
• Resistance to these agents develops frequently.
Pyrimidines

Pyrimethamine

Trimethoprim
• The mechanism of action of pyrimidines is different and their structures are not related to quinine and aminoquinolines.
• The sites of action for these derivatives include both the erythrocytic forms of P. vivax.
MOA
• Structurally, these derivatives resemble the pteridine portion of dihydrofolic acid (FH2)
• And interfere with its reduction to tetrahydrofolic acid (FH4) by dihydrofolate reductase, thereby interfering with the utilization of folic acid (in malarial protozoa)
• Pyrimethamine & trimethoprim are used in suppressive treatment and as radical cure agents.
SAR: -
• Maximum activity is obtained when an electron-donating group was present in the 6-position e.g alkyl.
• When a chlorine atom is present in the para-position of the phenyl ring a maximum activity is obtained.
• If the two rings are separated by either an oxygen atom or a carbon atom, antimalarial action is decreased. Eg. Trimethoprim
ADME: -
• Pyrimethamine is slowly but completely absorbed from the G.I.T.
• It is localized in the liver, the lungs, the kidney & the spleen.
• It is completely metabolized
• It is slowly excreted through the urine.
• Trimethoprim has a shorter half-life (24hrs) than pyrimethamine.
Toxicity: -
• Pyrimethamine is relatively nontoxic, but overdoses may lead to depression of cell growth by inhibition of folic acid activity.
Sulfones
• Dapsone:- 4,4’- diaminodiphenyl sulfone has a prophylactic activity against resistant P. falciparum.
• It is was developed for the treatment of leprosy.
• Dapsone act by competing with PABA, in the synthesis of folic acid.
• Dapsone has a prolonged duration of action and a moderate toxicity. Combination with pyrimethamine have been effective in suppressing symptoms of malaria due to chloroquine-resistant P. falciparum.

Sulfonamides
• Sulfonamides are used in antimalarial therapy against drug- resistant malarial strains.
• They are effective against erythrocytic stages of the malarial protozoa.
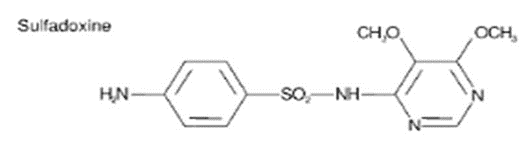
• Medium or long-acting sulfonamides are used clinically as antimalarials particularly sulfadiazine, sulfadoxine and sulfalene.
• Each of the above sulfonamides are much more effective when given in combination with pyrimethamine.
Sulfadoxine: -
Sulfalene: -

Sulfadiazine: -

Artesunate
• Artesunate is a medication used to treat malaria.
• The intravenous form is preferred to quinidine for severe malaria.
• Often it is used as part of combination therapy, such as artesunate plus mefloquine or amodiaquine.
• It is not used for the prevention of malaria

Artemether
• Artemether is used to treat acute uncomplicated malaria.
• It is administered in combination with lumefantrine for improved efficacy. This combination therapy exerts its effects against the erythrocytic stages of Plasmodium spp. and may be used to treat infections caused by P. falciparum and unidentified Plasmodium species.

Atovaquone
• Atovaquone is a naphthoquinone used for the prevention and treatment of Pneumocystis pneumonia (PCP) and,
• In combination with proguanil, used for prevention and treatment of P. falciparum malaria

Classification based on MOA
• Antimalarials can be divided into two classes based on their MOA
• 1) The first class of compounds are characterized by rapid onset of schizoticidal action
• Includes the cinchona alkaloids, aminoquinolines and acridines and involves a relatively non-specific mechanism.
• The derivatives in this first group inhibit nucleic acid and protein synthesis in the protozoal cell.
• Due to the interaction between the drug and DNA.
• The flat aromatic quinoline or acridine ring can position or intercalate between the base pairs in the DNA-α-helix and the secondary alcohol group in quinine or the amino groups in the other derivatives provide secondary binding through hydrogen bond formation.
• Because these events can take place in mammalian host cells as well as in parasite cells,
• The antimalarial action depends upon selective accumulation of the drugs in the parasite cell.
• E.g chloroquine, erythrocytic schizonts can concentrate the drug to a level many times that of the plasma concentration.
• Host cells require a 100-fold greater concentration to be affected than is necessary to kill parasite cells.
• 2) The second class includes the pyrimidines, biguanides and sulfones and involves interference with the synthesis of tetrahydrofolic acid (FH4).
• This mechanism is characterized by a slowly developing schizonticidal action dependent upon the stage of multiplication of the parasite.
• The pyrimidine and biguanide derivatives are competitive inhibitors of dihydrofolic acid (FH2), binding to dihydrofolate reductase and thereby interfering with conversion of FH2 to FH4. FH4 is necessary
• The effect occurs in host as well as in parasite cells, but is selective to the parasite because of a greater effective concentration.
• The sulfones as well as sulfonamides interfere with the synthesis of dihydrofolic acid by competing with p-amino benzoic acid (PABA) incorporation.
• The metabolites of the sulfones resemble PABA structurally and when incorporated, produce an inactive coenzyme.
• This mechanism does not operate in mammalian host cells.
0 Comments: