Sulfonamides and Cotrimoxazole
Sulfonamides and Cotrimoxazole
Content
Sulfonamides and Cotrimoxazole
• Classification
• Mechanism of action
• Pharmacokinetics
• Drug interactions
• Clinical uses
Objectives
At the end of this session, students will be able to:
• Classify sulfonamides
• Describe the mechanism of action of sulfonamide and cotrimoxazole
• Outline the adverse effects of sulfonamides and cotrimoxazole
• Discuss the therapeutic uses of sulfonamide and cotrimoxazole
Sulfonamides and Cotrimoxazole
• Sulfonamides are structural analogues of p-amino benzoic acid (PABA)
• Obtained from sulphanilamide
• -NH2group is responsible for antibacterial property
Classification of sulfonamides
Orally absorbable agents
• Short acting sulfonamides (t1/2 6-9 h)
– Sulfacystine, Sulfadiazine, Sulfisoxazole and Sulfamethizole
• Intermediate acting sulfonamides (t1/2 10-12 h)
– Sulfamethoxazole and Sulfamoxole
• Long acting sulfonamides (t1/2 7-8 days)
– Sulfadoxine
Orally non absorbable agents
• Sulfasalazine
• Olsalazine
• Balsalazine
Topical agents
• Silver sulphadiazine
• Mafenide
• Sulfacetamide
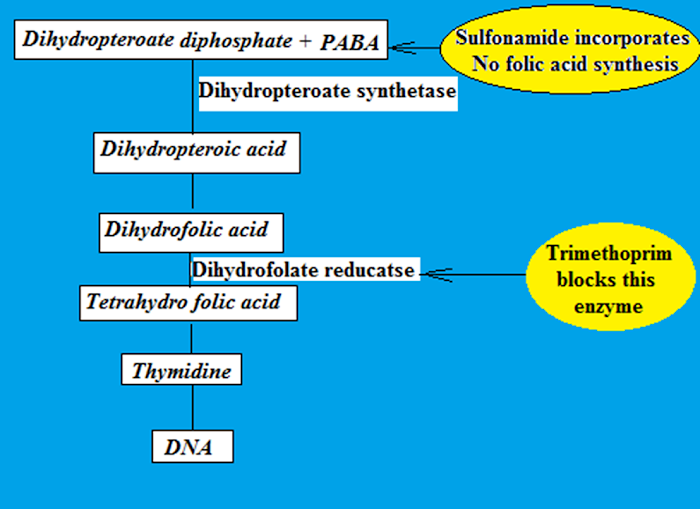
Mechanism of action
• Bacterium synthesizing its own folic acid are more susceptible
• Inhibits formation of tetra hydro folic acid
• Sulfonamides are structurally similar to PABA
• May lead to synthesis of false folic acid
• False folic acid metabolically injurious to bacteria
Mechanism of action of sulfonamides

• Antibacterial effect of sulfonamides can be overcome if excess of PABA is present (Puss)
• Puss contains tissue breakdown product thymidine
• Thymidine could be used by bacteria to bypass the need of folic acid
Cotrimoxazole
• Combination of sulfamethoxazole + trimethoprim (5:1)
• Has wider spectrum of activity
• Delays development of bacterial resistance
• Synergistic action is due to blockade of folic acid syntheis at two sites
• Sulfonamides inhibits dihydropteric acid synthase
• Trimethoprim inhibits dihydrofolate reductase
Antimicrobial spectrum
• Bacteriostatic to gram positive and gram negative
• Attain bactericidal concentration in urine than in body fluids
Susceptible organisms
E. coli, Shigella, Salmonella, Haemophillus influenzae, Vibrio cholerae, Proteus, Neisseria gonorrhoeae, N. meiningitidis, Actinomycetes, Rickettsiae, Toxoplasma gondii
Resistance
Mutations leading to
• Overproduction of PABA
• Alteration in the nature of DHP synthase enzyme
• Increased capacity to inactivate the drug
• Inhibition of drug accumulation
• Alternate metabolic pathway for the synthesis of essential nutrients
Pharmacokinetics
• Well absorbed when given orally
• Peak plasma concentration attained in 4-6 hours
Distribution
– well distributed
– 10-95% plasma protein bound
– In unbound form enters into body fluids like pleural, peritoneal and synovial
– Sulphdiazine & Sulfisoxazole – enters CSF
Metabolism
• In liver
• By acetylation
• Acetylated derivative responsible for side effects
• Accumulates in acidic urine – crystalluria
Excretion – Kidneys
Pharmacokinetics of cotrimoxazole
• Attains plasma concentration ratio of 20:1
• Trimethoprim – high entry into tissues ; less available in plasma
• Metabolised in liver
• Excreted through kidneys
• Half-life is 10 h
• Peak plasma level – Trimethoprim – 2 h and Sulphamethoxazole – 4 h
Adverse effects
• Nausea, Vomiting, epigastric pain, crystalluria
• Haemolytic anaemia, Agranulocytosis and aplastic anaemia
• Hypersensitivity reactions
• Kernicterus – bilirubin deposited in brain- encephalopathy (new born)
• Contraindicated in pregnant women and lactating mothers
Drug interactions
• Sulfonamides are enzyme inhibitors
• Inhibit the metabolism of certain drugs
• Increases activity of
– Oral anticoagulants
– Sulfonyl ureas (Antidiabetics)
– Anticonvulsants
Clinical uses
Orally absorbable sulfonamides
• Acute uncomplicated UTI – sulfisoxazole
• Gum infection
• Streptococcal pharyngitis
Topical
• Sodium sulfacetamide – eye drops in conjuctivitis
• Silver sulfadiazine – infection – in burn cases
• Mefanide – effective against gram positive and gram negative bacteria
Sulfasalazine – Ulcerative colitis
Cotrimoxazole
• Chronic UT infection
• Bacterial respiratory infection – chronic bronchitis
• GI infections- Typhoid, bacterial dysentry, diarrhoea
• Prostrate inflammation
• STDs
• Pneumonia
Summary
• Sulfonamides are structural analogues of p-amino benzoic acid (PABA) obtained from sulphanilamide
• Sulfonamides show antibacterial action via inhibition of THFA formation
• Sulfonamides are classified based on duration of action into short acting, Intermediate acting and long acting sulfonamides
• Cotrimoxazole is a synergistic combination of sulfanethoxazole and trimethoprim - used in the treatment of many infectious diseases

0 Comments: